The Food and Drug administration is responsible for approving prescription and non-prescription drugs for use. This is done through one of the six centers in the FDA called the Center for Drug Evaluation and Research. The other centers are responsible for medical and radiology devices, food and cosmetics, biologic agents, veterinary drugs and tobacco products. Since 1992 over 1,000 new prescription drugs have come to market. So far in 2016 there have been 6 new drugs and in 2015 there were 45. Over the counter medications are handled differently than prescription medicatons. In those cases the FDA only reviews the active ingredients. There are over 30,000 non-prescription drugs on the market.
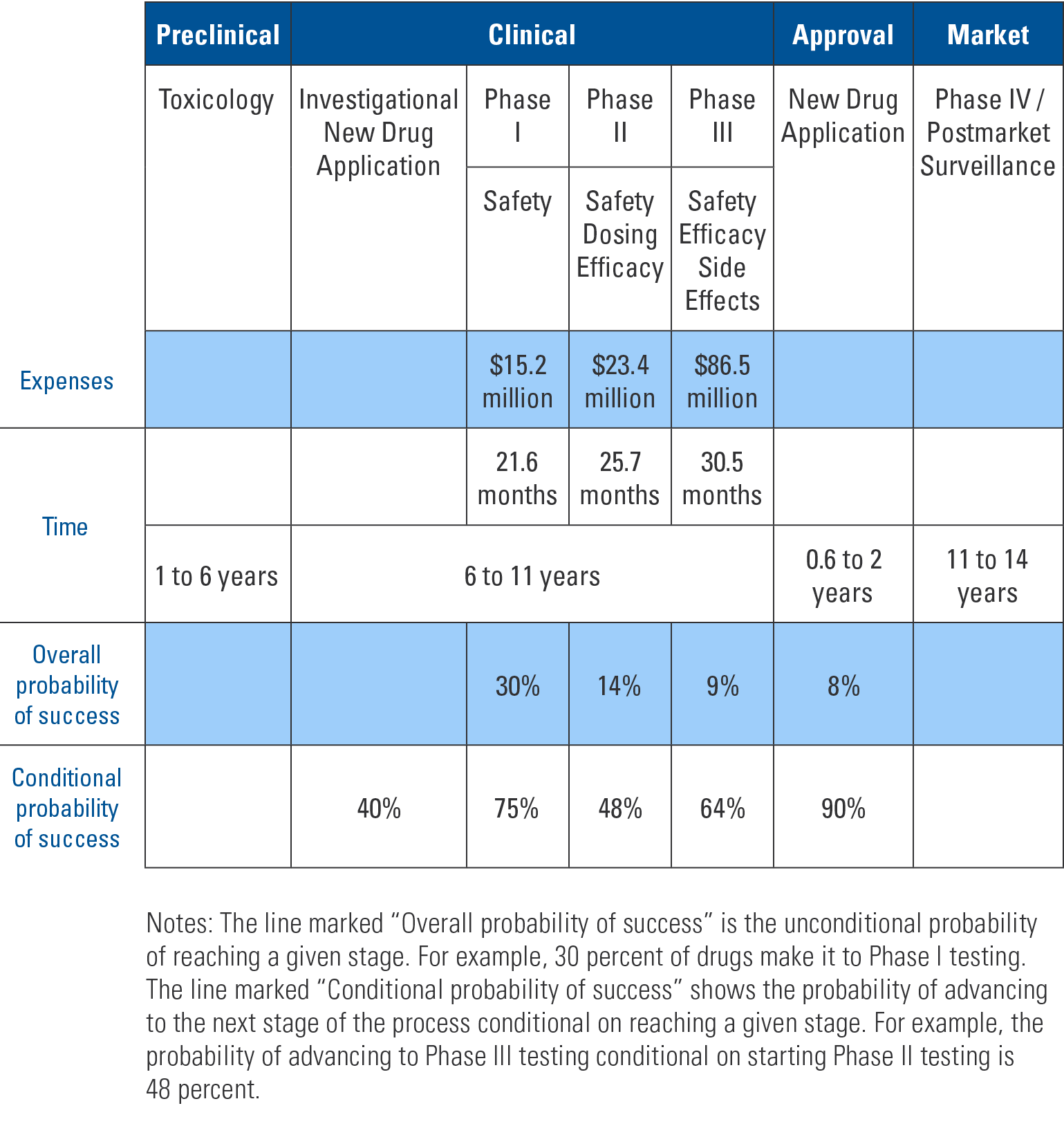
The table below shows the process, cost and time required for new prescription drug approval. Compounds that potentially have pharmacologic effect are studied in animal models. If they prove promising then an investigational new drug (IND) application is submitted. The FDA has 30 days to review the application and, if needed, put a “clinical hold” on the process to discuss concerns with the applicant. An IND is required to do phase I studies in humans. Phase I studies determine if the compound is safe in humans, side effects and the metabolism and excretion mechanisms. Typically 20-80 healthy volunteers are used.
An Overview of the Drug Development Process
Additionally, before any clinical trial can be done, each study must be approved by an institutional review board (IRB). The IRB is not overseen by the FDA but rather the institution at which the trial is to be performed. The panels are comprised of medical and lay people. They review the studies to ensure safety to participants and that adequate informed consent is obtained.
If phase I studies are positive then phase II studies begin. This phase examines effectiveness of the drug for particular conditions. The drug is compared to either placebo or a similar drug already on the market. These studies involve around 300 participants. Again, if results are positive, then phase III trials are performed. The FDA and drug sponsor agree on large-scale studies to determine safety and effectiveness. Typically trials consist of a few hundred to 3,000 people.
–
“Once a drug is approved it must also undergo phase IV post-marketing surveillance. This is to ensure that when used on a wider population the drug does not cause previously unfound side effects and further verify efficacy.”
After successful phase III studies, a new drug application (NDA) is submitted to the FDA. This application reviews manufacturing specifications, drug stability and bioavailability for each of the dosage forms. Also reviewed are results of toxicological studies and the packaging and labeling for both consumers and prescribers. The goal of the FDA is to decide within 60 days if the NDA can be filed or is incomplete. If filed, the application with all previous studies is sent to committee for final decision. Inspection of the manufacturing facilities is included as part of this NDA process.
Once a drug is approved it must also undergo phase IV post-marketing surveillance. This is to ensure that when used on a wider population the drug does not cause previously unfound side effects and further verify efficacy.
As shown in the table, most compounds do not make it past initial animal studies and even those that do face a steep uphill battle to pass subsequent stages. Even with such rigorous pre-market testing some approved medications are shown to cause harm or not be effective in phase IV surveillance and are withdrawn from the market.
One of the best ways to limit antibiotic resistance is to decrease antibiotic use. Most infections either are not or cannot be cultured before deciding on the need for antibiotic treatment. Therefore, the conundrum is avoiding prescriptions for non-bacterial infections while not missing antibiotic treatment when needed. Physicians are also concerned about patient perceptions and satisfaction with care, which leads to more prescriptions than necessary. In 2010, there were 258 million courses of antibiotics which is equivalent to 833 prescriptions per 1,000 people.
–
“Each year in the United States, 41.2 million prescriptions are written for acute respiratory infections — of which half are inappropriate.”
Generally, upper respiratory infections are viral. Even most sinusitis and bronchitis are self-limited when bacterial, and symptoms should resolve in 10–14 days without treatment. Moderate to severe infections may warrant antibiotics. Each year in the United States, 41.2 million prescriptions are written for acute respiratory infections — of which half are inappropriate. 69% of acute adult respiratory infections were treated with antibiotics during the winter of 2009–2010.
In one study, a signed-commitment poster with a picture of the physician along with a letter explaining reasons and commitment to responsible prescribing was put in the exam room for three months. Prescription antibiotic use decreased almost 20% compared to a control group of physicians without the posters in their exam rooms.
A British study examined immediate versus delayed antibiotic prescriptions for respiratory infections. There were no statistical differences in symptom severity, duration or temperature. 97% of the immediate-prescribed antibiotics were taken compared with 33–39% in various delayed-arm strategies. People who used antibiotics in the delayed-arm took them four days later. The study concluded that delayed prescribing helps to decrease antibiotic use while not causing any harm and with no significant effect on patient satisfaction.
These studies show there are various ways to decrease antibiotic use. This will help slow the emergence of resistant bacteria.
Caregivers are a vital part of maintaining health for others, regardless of age. Merriam-Webster defines a caregiver as a person who gives help and protection to someone who is sick. This definition can also be expanded to a person who gives help and protection to another person. Caregivers are not only providers, but they also are recipients of care. Their role puts them at risk for health conditions of their own.
One study of primary family caregivers showed that 44% suffered from anxiety and depression, 15% pre-loss grief, and 10% from moderate to severe levels of demoralization. Caregivers often have poor sleep patterns as they “keep one eye open” at all times. Even caregivers who do not live with their charge do not sleep well as they are hypervigilant about the phone ringing with an issue.
–
“Caregivers are not only providers, but they also are recipients of care. Their role puts them at risk for health conditions of their own.”
Caregiver access to the ill person’s medical information can be difficult as hospitals and offices may not grant information access to the caregiver. As the issue is more broadly recognized, this is beginning to change. If able, the sick person should have durable power of healthcare documents on file with the institutions or specifically sign a release to allow sharing of medical information.
The Advisory Committee on Immunization Practices (ACIP) met July 22, 2021 to review data regarding COVID booster vaccinations for immunocompromised people. This is a summary of the that meeting, and the slides from the meeting are attached as well.
On August 12, 2021 the FDA approved COVID vaccinations for a third booster injection in immunocompromised people. This was the first step towards booster vaccinations. Today, the Advisory Committee on Immunization Practice (ACIP) meets to review the data to make recommendations regarding specifics about timing and who should receive the booster.
The recommendations are expected to follow discussion at the July 22nd meeting of the ACIP. There are two main questions to be answered. Who is considered immune compromised and timing of the booster dose.
For the purposes of this discussion, immunocompromised people are only 2.7% of the US population. Categories are likely to include stem cell and solid organ transplant recipients, people with hematologic and solid organ cancers, severe primary immunodeficiencies, people living with HIV, people being treated with cancer chemotherapy, tumor necrosis factors, certain biologic agents such as rituximab and people being treated with high dose steroids. High dose steroids are defined as prednisone 20 mg daily or more for more than 2 weeks. The definition may include people with chronic renal failure or advanced kidney disease, dialysis patients, patients with nephrotic syndrome or people with lack of a functional spleen.
Studies so far have shown that the vaccines are between 71-80% effective to prevent COVID infection in the immunocompromised compared to 90% in the non-immunocompromised after 2 doses. They have also shown 75% effectiveness compared to 94% effectiveness respectively for symptomatic COVID infection. Prevention of COVID hospitalizations have been 59% and 91% respectively among the two groups.
The ACIP has quoted four studies ranging in size from 30 to 106 people regarding effectiveness of third doses. In those studies people who were antibody negative after two doses of vaccine were then tested after a third dose. Between 33% and 50% or people converted and had antibodies after the third dose.
Currently the recommendation is not to test for antibodies or cellular immune testing (T-cell tests) are not recommended. This recommendation may change in the future.
More communication will follow after the ACIP meets to make their recommendations. At this time the discussion is about immunocompromised people only. Expectations are that booster doses for everyone will be recommended in the future. Efficacy of the vaccine for the general population has been shown to persist for over 8 months so far.
We are proud to report that our office delivered over 1400 vaccine doses with the first round. This compares to large institutions such as Rush Medical Center that gave out 100,000 doses during the same period. For comparison purposes, our office is a staff of four compared to theirs of 12,000.
There are increasing reports in the news media about the coronavirus and its spread. While it is important to stay informed, there is no reason to panic. To put it in perspective, current data suggests that the mortality rate for those infected with coronavirus is about 2%, while for the current influenza season, the percentage of deaths related to influenza and pneumonia is 6.8% (data from the Centers for Disease Control and Prevention). The threshold for calling infections an epidemic is 7.3%.
As of February 25, 2020, in the United States 416 people have been tested for coronavirus and there are 14 confirmed cases — 12 from travel and two from person-to-person spread, but no reported deaths. On average, there are between 30,000 and 50,000 deaths each year in the United States that are attributable to influenza.
–
“If you have symptoms and believe you are at risk of coronavirus infection, call your doctor before going in. The determination will then be made as to the best course of action. Home treatment is appropriate for some people, but not for others.”
A few things to know:
The virus is spread by respiratory droplets. This means that coughing and sneezing spread the illness. Handwashing and covering one’s mouth when coughing and sneezing helps prevent transmission.
Wash hands with soap and water for at least 20 seconds or use alcohol-based hand sanitizers with at least 60% alcohol content.
The virus presents with fever, cough and shortness of breath. The current belief is that people with these symptoms and who travel or have had known contact with recent travelers are at risk.
If you have symptoms and believe you are at risk of coronavirus infection, call your doctor before going in. The determination will then be made as to the best course of action. Home treatment is appropriate for some people, but not for others.
There is no known medication for treatment at this time. The recommended treatment is supportive care.
As cases continue to grow globally, it is expected that more travel advisories and restrictions will occur. According to the CDC site as of February 27, China and South Korea are at a warning level 3 which means to avoid all non-essential travel. Iran, Italy and Japan are at an alert level 2. Older adults and people with chronic medical conditions should consider postponing non-essential travel. The CDC has Hong Kong at a watch level 1 and usual precautions are indicated.
Also as of February 27, Singapore, Thailand and Taiwan are other places with potential for community spread of the disease. All of these recommendations are changing rapidly as more cases are identified.
Update 3/1/2020
The number of cases in the United States continues to increase with one report now at 74 cases nationally including 3 presumptive cases in Illinois. As the U.S. has a limited supply of test kits, and there is evidence of community spread, the number of infected people is likely higher. Likewise, the death rate is likely lower than reported given mild and un-diagnosed cases. As of now, no updated numbers are on the CDC website.
Anyone with symptoms such as fever, cough and shortness of breath should stay home and avoid work, school or public places including public transportation, ride-sharing or taxis. Persons with symptoms should also avoid others in the home. The CDC recommends staying away from pets although no transmission to or from pets has been documented. The World Health Organization does not recommend isolation from pets.
The incubation period (time of exposure until symptoms) is between one and fourteen days with an average of five days.
Decision to travel should take into account destination and current state of knowledge. Additional consideration should be given to potential risk from quarantine and difficulty returning.
Update 3/3/2020
The CDC is now only updating their website on Mondays, Wednesdays and Fridays. Projections are that there will be up to one million test kits available in the United States in the next 1-2 weeks. This is compared to the few thousand tests that have been available so far. As a result it is reasonable to expect a large number of new cases to be diagnosed.
According to an editorial in the Journal of the American Medical Association last week, preliminary data show the incubation period may be up to 24 days and the potential secondary cases from a single infected person is two or three people.
Based upon 4 patients in China, it may be possible that some patients who have clinically recovered from the disease continue as carriers.
It remains to be seen how much information will be reported by the CDC as new information emerges. We will need to rely on other credible sources in addition to any CDC reports.
Update 3/8/2020
The CDC is now back to updating their website daily on weekdays. The one million test kits promised have not materialized but continue to be promised. There are varying reports of the number of tests available and the actual number completed. There are approximately 105,000 cases worldwide with over 500 suspected or confirmed cases in the United States. There is limited new guidance from the CDC and continues to be conflicting reports from the government.
As spring break is fast approaching for many people, there are questions about what to do with plans. Other than the countries previously listed there are no new countries on the watch list. It is still expected that new cases will be found worldwide. Over 100 countries are now affected. Although not an official recommendation, I would advise against international travel. Domestic travel should be considered on an individual basis. Older people and people with underlying cardiac, pulmonary, diabetic or immuno-suppressive illness are at higher risk of contracting more severe disease. It would also generally be reasonable to avoid large gatherings which has been arbitrarily defined as over 50 people.
The World Health Organization is also producing daily situation updates which can be found at:
As expected the number of cases is growing. This trend will continue and likely accelerate here in the United States as more testing comes on-line.
A research letter in Jama published on March 11 looked at 205 patients who had multiple specimens taken. Virus was found broncho-alveolar lavage specimens, nasal swabs, pharyngeal swabs, feces and rarely blood. No virus was found in urine. This information furthers our knowledge about the virus and re-enforces the need for proper hygiene.
Governor Pritzker has ordered all Illinois schools closed until March 30. It remains important that everyone avoid large gatherings in order to contain spread of the disease and avoid personal illness. There is no defined number of a large gathering. It now seems that 50 is too large for the definition. Perhaps 10-15 is a better number to use, but this also should take into account the distance between people. Six feet is considered a safe distance to avoid spread of the virus.
It is prudent to avoid non-essential travel, particularly long-distance travel. If you are unsure of your plans, you should consult a physician.
No one can accurately predict the duration of the outbreak, but with proper measures, it could be contained, not eradicated, in a few months. This is based upon experiences in China. Here in the United States we will likely follow the path of China and Europe.
During this time of increased stress it is important to still think about general health. Do not stop chronic medications and if unsure about taking over the counter medications, consult your physician. Physical activity remains important for physical and mental health. While I recommend avoiding health clubs, walking, running, biking and other outdoor or home based exercise is another way to maintain activity.
COVID-19 Fact Sheets from the Centers For Disease Control and Prevention (CDC)
What you need to know about coronavirus disease 2019 (COVID-19) Download PDF
What to do if you are sick with coronavirus disease 2019 (COVID-19) Download PDF
Although we think of antibiotics as benign, one in five emergency room visits are for antibiotic-adverse effects. These include allergic reactions, clostridium dificile infection and drug interactions. Good hygiene decreases risk of infection.
–
“We need some bacteria for normal function so our aim should not be to eradicate all bacteria. Just as with the rest of the world there is an ecological balance that is beneficial.”
When soap and water are not available, alcohol-based hand sanitizers are a good alternative. Sanitizers with 60-95% alcohol are more effective than less potent or non-alcohol based products. The less potent products may also promote resistance by reducing but not killing the bacteria. They also cause more skin irritation. Heavily soiled or greasy hands should be cleaned with soap and water as other sanitizers become less effective in these settings. Of note, alcohol hand sanitizers are not effective against clostridium dificile.
We need some bacteria for normal function so our aim should not be to eradicate all bacteria. Just as with the rest of the world there is an ecological balance that is beneficial. Fighting antibiotic resistance is a battle that will never be won, but there are steps we can all take to limit the problem of resistant pathogenic bacteria.