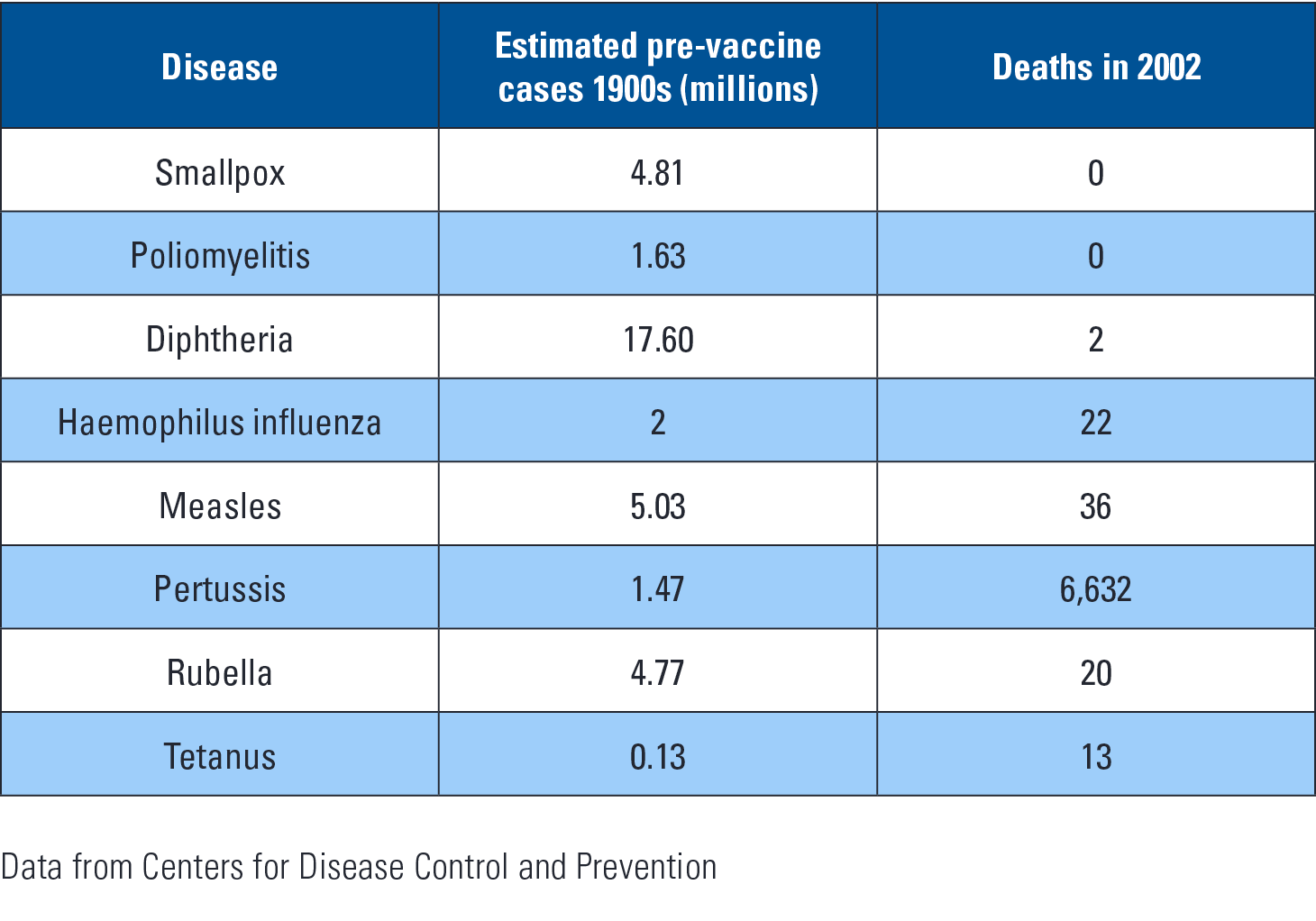
Vaccines are the most cost effective way to save lives and preserve health. The first vaccine was developed by Edward Jenner in 1796. He noted that milkmaids exposed to cowpox did not get smallpox. In the twentieth century 375 million people died from smallpox. Due to the effectiveness of the vaccine, no one has died of smallpox since 1978. Vaccines help decrease unnecessary antibiotic use by preventing disease that could lead to inappropriate antibiotic prescriptions.
We now have more than 70 vaccines which are good against 30 different pathogens. The table below shows vaccine effectiveness for common diseases. Despite vaccine success there are many barriers to development, production, and deployment.
Some microbes, such as HIV, tuberculosis, and malaria have been particularly difficult to design vaccines against, so 4 million people still die each year of these diseases. The usual way to develop vaccines is to use measurement of antibody response as a marker for effectiveness. Due to progress in molecular biology, we can now develop vaccines based upon specific binding sites. This is being done for HIV and influenza. If successful, there may be a universal flu vaccine that does not require annual treatment against our best estimate of the year’s likely strains. Influenza vaccines can now be made from cell based and recombinant methods rather than relying on egg based cultures.
–
“Vaccines help decrease unnecessary antibiotic use by preventing disease that could lead to inappropriate antibiotic prescriptions.”
Deployment of vaccines to people in need remains an enormous challenge. In developing countries three children die each minute of a vaccine preventable illness. As we are hearing with the Ebola epidemic, even when help is available people do not trust the healthcare system.
In summary, we have made great strides in preventing disease and will continue to do so as vaccination technology improves.